|
||||||||||||
#冠動脈の血流の層流乱れを、#非観血、簡易的に検知 (薬事未認可に付き注意) |
||||||||||||
|
||||||||||||
|
||||||||||||
|
||||||||||||
|
|
||||||||||||
#冠動脈の血流の層流乱れを、#非観血、簡易的に検知 (薬事未認可に付き注意) |
||||||||||||
|
||||||||||||
|
||||||||||||
|
||||||||||||
|
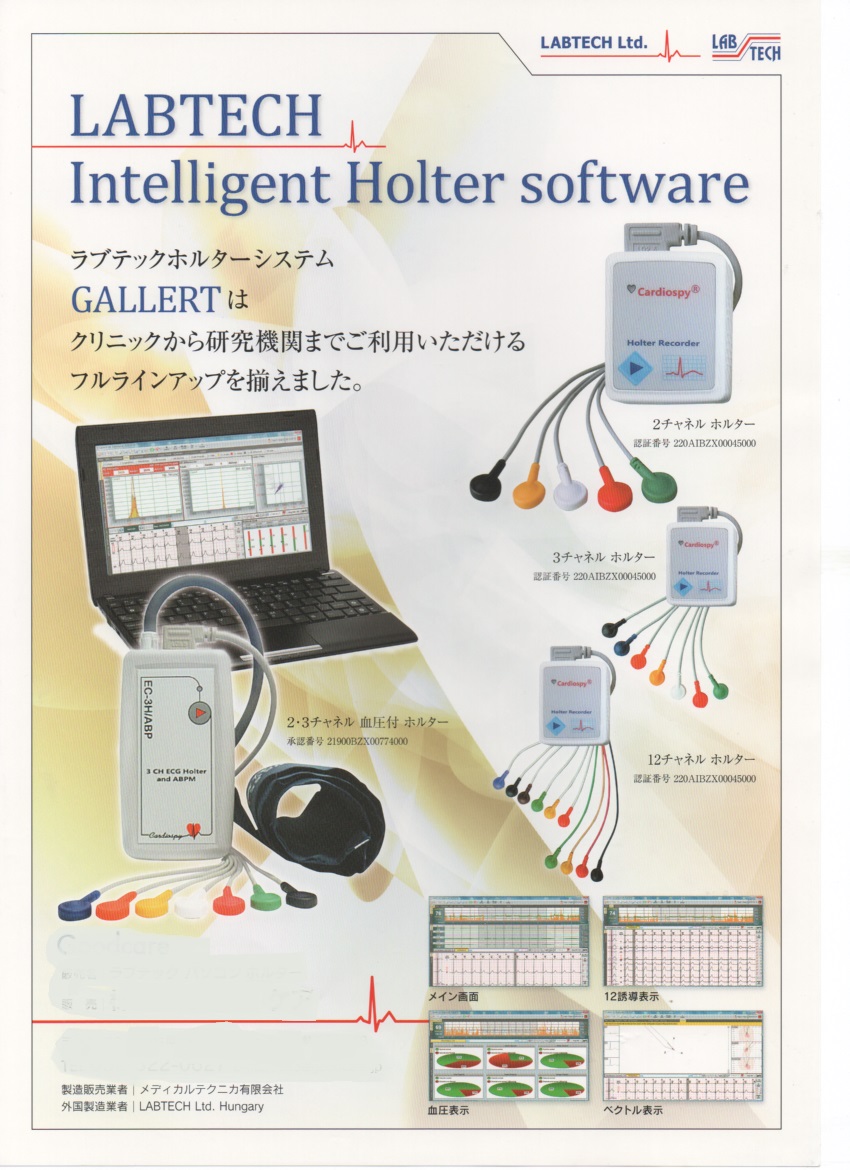
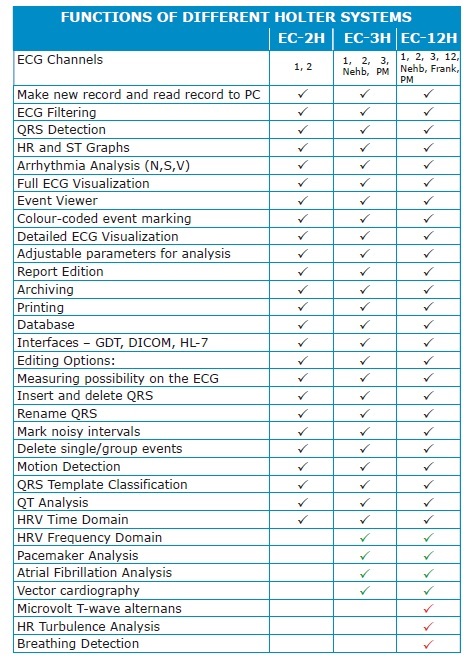
PCの機能が向上し、#Descrete_Wavelet 手法が、お求めやすい低価格で 実現し、#心房のP波を自動検出できるようになりました、 #心房細動の自動解析能をお試し賜われれば幸いです 臨床用 #薬事認可済 |
||||||
#Labtech社は、当社独自の方法による #P波自動検出と #心房細動自動解析手法と #T_Wave_Alternans 解析手法を開発し、当社ホルターに搭載。 |
||||||
#VectraCardiology, #Heart_Rate_Variability , #TWA_オルタナンス #Turbulence、#3D可変表示、#Spectral_Analysis等が装備 |
||||||
|
||||||
| #先天性心疾患の教科書 #Pedcath8 | ||||||
|
||||||
|
|
||||||
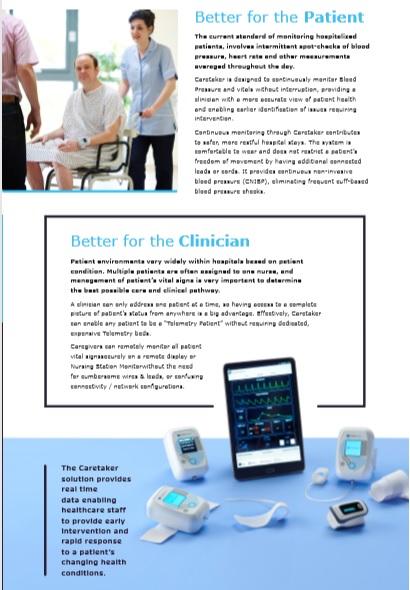
#ケアテイカメディカル社ー#研究用 #非観血血圧・#連続解析観血血圧計 ・#ポータブル・#ウエアラブル・#一拍毎解析出力付き |
||||||
|
httpswww.ncbi.nlm.nih.govpmcarticlesPMC5361833 BMC Anesthesiol. 2017; 17: 48. Published online 2017 Mar 21. doi: 10.1186/s12871-017-0337-z PMCID: PMC5361833 PMID: 28327093 #Continuous_Non-invasive_fingercuff #CareTakerR comparable to invasive intra-arterial pressure in patients undergoing major intra-abdominal surgery Irwin Gratz,1 Edward Deal,1 Francis Spitz,1 Martin Baruch,2 I. Elaine Allen,3 Julia E. Seaman,4 Erin Pukenas,1 and Smith Jean1 Author information Article notes Copyright and License information Disclaimer This article has been cited by other articles in PMC. Associated Data Data Availability Statement The datasets generated during and analysed for the current study are available from the corresponding author on reasonable request. Abstract Background Despite increased interest in non-invasive arterial pressure monitoring, the majority of commercially available technologies have failed to satisfy the limits established for the validation of automatic arterial pressure monitoring by the Association for the Advancement of Medical Instrumentation (AAMI). According to the ANSI/AAMI/ISO 81060?2:2013 standards, the group-average accuracy and precision are defined as acceptable if bias is not greater than 5 mmHg and standard deviation is not greater than 8 mmHg. In this study, these standards are used to evaluate the CareTakerR (CT) device, a device measuring continuous non-invasive blood pressure via a pulse contour algorithm called Pulse Decomposition Analysis. Methods A convenience sample of 24 patients scheduled for major abdominal surgery were consented to participate in this IRB approved pilot study. Each patient was monitored with a radial arterial catheter and CT using a finger cuff applied to the contralateral thumb. Hemodynamic variables were measured and analyzed from both devices for the first thirty minutes of the surgical procedure including the induction of anesthesia. The mean arterial pressure (MAP), systolic and diastolic blood pressures continuously collected from the arterial catheter and CT were compared. Pearson correlation coefficients were calculated between arterial catheter and CT blood pressure measurements, a Bland-Altman analysis, and polar and 4Q plots were created. Results The correlation of systolic, diastolic, and mean arterial pressures were 0.92, 0.86, 0.91, respectively (p?<?0.0001 for all the comparisons). The Bland-Altman comparison yielded a bias (as measured by overall mean difference) of ?0.57, ?2.52, 1.01 mmHg for systolic, diastolic, and mean arterial pressures, respectively with a standard deviation of 7.34, 6.47, 5.33 mmHg for systolic, diastolic, and mean arterial pressures, respectively (p?<?0.001 for all comparisons). The polar plot indicates little bias between the two methods (90%/95% CI at 31.5°/52°, respectively, overall bias?=?1.5°) with only a small percentage of points outside these lines. The 4Q plot indicates good concordance and no bias between the methods. Conclusions In this study, blood pressure measured using the non-invasive CT device was shown to correlate well with the arterial catheter measurements. Larger studies are needed to confirm these results in more varied settings. Most patients exhibited very good agreement between methods. Results were well within the limits established for the validation of #automatic_arterial pressure monitoring by the AAMI. Keywords: Non-Invasive, CareTaker, Central_blood_pressure_, Finger_cuff, Intra-Arterial pressure |
||||||
|
||||||
|
||||||
| |
| お問い合わせ先 メディカルテクニカ有限会社 | ||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
| Medical Teknika add link | Medical Teknika add link | Medical Teknika add link | Medical Teknika add link |
|---|---|---|---|
| Medical Teknika add link | Medical Teknika add link | Medical Teknika add link | Medical Teknika add link |
| Medical Teknika add link | Medical Teknika add link | Medical Teknika add link | Medical Teknika add link |
| Medical Teknika add link | Medical Teknika add link | Medical Teknika add link | Medical Teknika add link |
| Medical Teknika add link | Medical Teknika add link | Medical Teknika add link | Medical Teknika add link |
| Medical Teknika add link | Medical Teknika add link | Medical Teknika add link | Medical Teknika add link |